What is CAH
Introduction
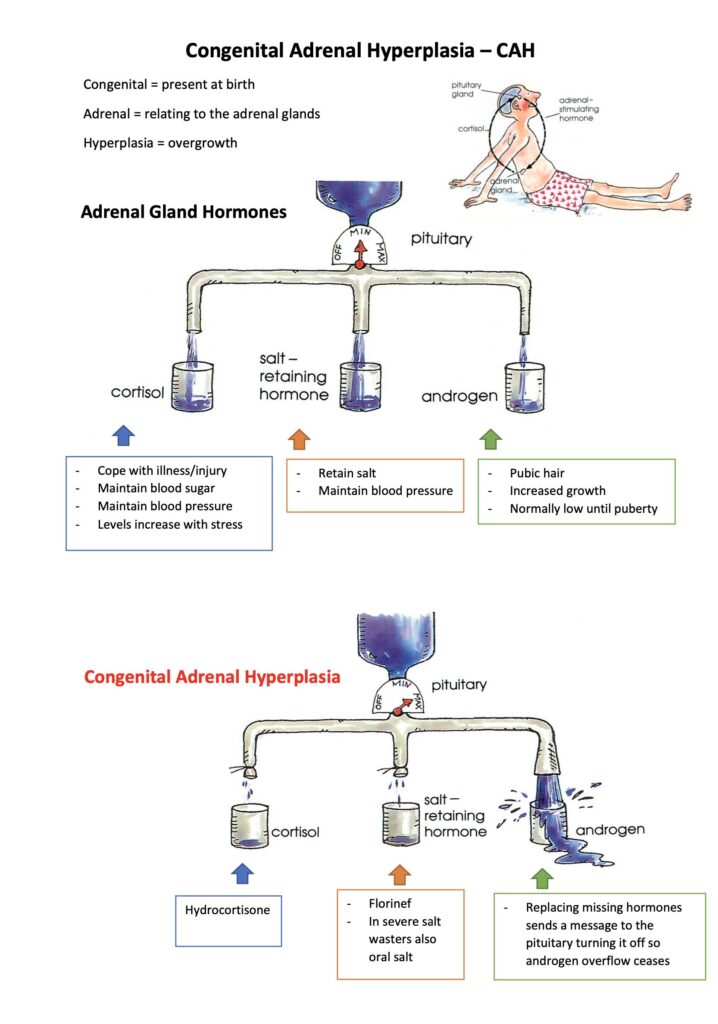
Congenital Adrenal Hyperplasia (CAH) is a condition, which affects the production of hormones from the adrenal gland. “Congenital” means present at birth: “Adrenal” means adrenal glands: “Hyperplasia” means enlarged.
Children born with this condition have an enzyme deficiency, which interrupts the normal production of the hormones from the adrenal gland. There is both cortisol and aldosterone deficiency, and an over stimulation of other hormones called androgens, with all causing significant health issues for the child. Management is through replacing the missing hormones and suppressing the excess androgen production, with more specific management required during times of illness.
There is a range of challenges faced by parents of children with this diagnosis. A family’s adjustment can be greatly enhanced through counseling, education and support of experienced health professionals. Health education strategies are important in facilitating both understanding, and confidence to manage the condition and any health issues when they occur.
Diagnosis:
CAH is an inherited condition where both parents carry a faulty gene. There is a 1 in 4 chance in every pregnancy of having an affected child with the autosomal recessive inheritance. The incidence is 1:15,000 in Caucasian populations and but 1:6,000 in the Asian Sub-continent (Vietnam, Indonesia) and also in African populations.
Girls are diagnosed soon after birth as they present with virilised genitalia requiring immediate diagnostic investigations. The diagnosis is usually established within a few days of birth. Unfortunately, without newborn screening, boys show no signs of the possible diagnosis until about a week after birth, when they become progressively unwell, with an impending adrenal crisis. There is a significant history of poor feeding, lethargy and significant weight loss, which can eventuate in a state of collapse and death.
CAH may also present later in childhood, with an increased growth rate, an advanced bone age, appearance of pubic hair, excessive oiliness of the skin and hair, acne and progression into early puberty. These signs result from an excess secretion of androgen from the adrenal gland.
Management:
Medical Management:
Both cortisol and aldosterone are hormones essential for life. Treatment of CAH includes the replacement of the missing hormones with oral medication, and suppression of the excess androgen through adequate dosing regimens. Both children and adults with CAH are at risk of a salt losing ‘adrenal crisis’ in times of poor compliance, or during period of increased periods of stress in the body. This usually occurs during times of significant illness and injury, and during procedures requiring anaesthesia. On very rare occasions it could occur during periods of extreme emotional distress.
Treatment is required lifelong, with close supervision under the care of a specialized healthcare team. Regular management includes assessment of growth and development during childhood and physical examinations to assess for early pubertal development, and also includes bone age assessment and regular blood tests.
Psychological management:
There is an urgent need to manage the psychological impact of the diagnosis of CAH. The grief process experienced by parents can be overwhelming as they come to terms with the loss of their imagined healthy child. The psychological impact and issues are significant including,
- Virilised genitalia requiring gender determination.
- Diagnosis of a life threatening, life long condition.
- Implications of a genetically inherited condition and plans for future pregnancy
- Importance of compliance with life saving essential medications
- Emergency management strategies and sick day care to prevent an adrenal crisis
- Regular medical check-up, blood tests, examinations.
- Monitoring and compliance to ensure normal growth and development
- Navigating Puberty at an age appropriate time, gender identity for some and balancing hormonal issues at this time.
- Management of puberty and genital surgery for girls.
- Ethical implications relating to reconstructive surgery.